A young footballer tears his Achilles tendon, and the doctor's prognosis is grim: six months of rehabilitation. A friend advises him: "Try peptides, you'll be fit in two months."
In gyms around the world - especially in the US - peptides have become a phenomenon. They promise almost everything: faster healing, muscle building, fat loss. Names like BPC-157, TB-500, MK-677, or semaglutide are tossed around in every other discussion.
But what is the reality?
Let's take a look together at what peptides actually are, whether peptides for weight loss really work, and what information we currently have regarding their effects and side effects.
What are peptides
Basic definition of peptides
Peptides are short chains of amino acids linked by peptide bonds. If you imagine amino acids as LEGO bricks, peptides are small structures made up of 2 to 50 bricks.
These compounds occur naturally in the human body and fulfill a variety of biological functions - from transmitting signals between cells to regulating hormonal processes. Some of these molecules function as hormones, while others act as neurotransmitters or growth factors.
The difference between peptides, proteins, and hormones
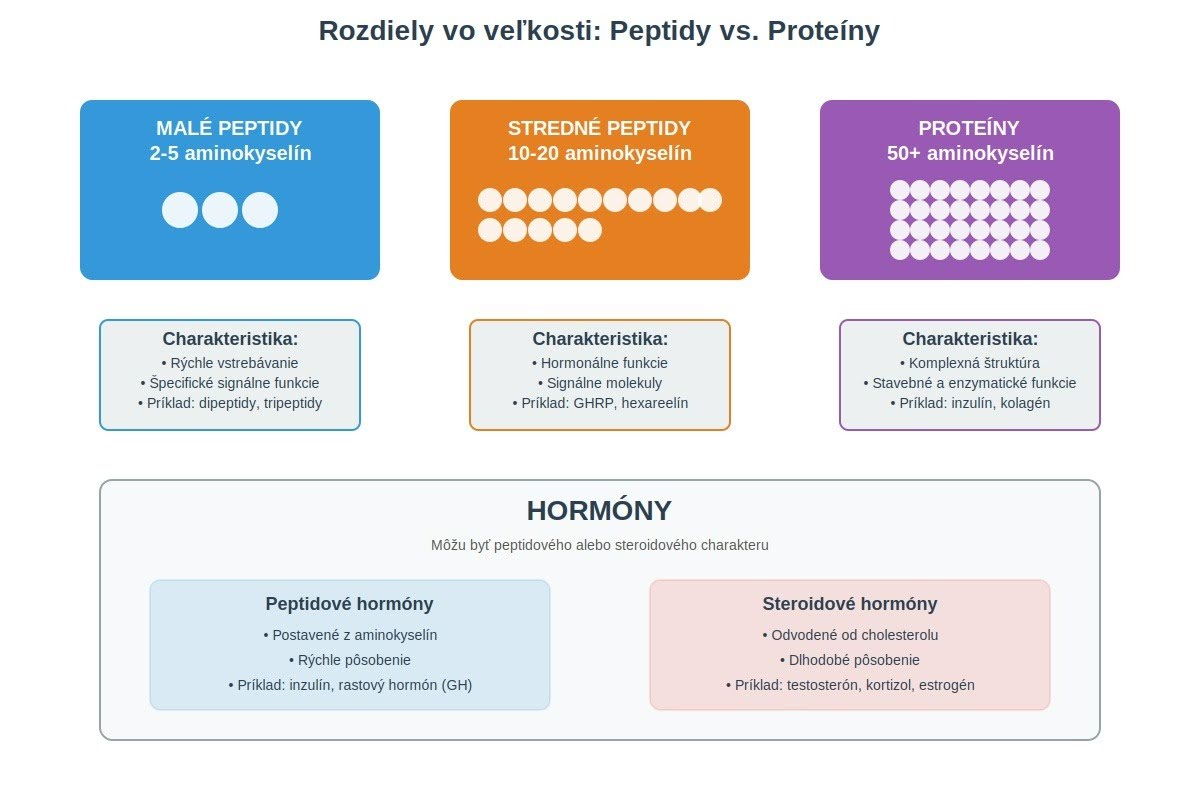
Even though all three categories consist of amino acids, they differ in size and function:
Peptides: 2-50 amino acids, they absorb quickly and have specific signaling functions.
Proteins: More than 50 amino acids, a more complex structure, structural and enzymatic functions.
Hormones: Can be peptide-based (insulin, growth hormone) or steroid-based (testosterone, cortisol).
Created using Claude AI (Anthropic)
The key practical difference: larger proteins are broken down into amino acids in the digestive tract, whereas smaller peptides can pass into the bloodstream intact—remaining in their original state and functioning as a whole.
Why Peptides Are Studied in Medicine and Sports
Medical research focuses on peptides for two reasons. First, they can be highly specific in their action; they are able to bind to precisely defined receptors without affecting other systems. Second, the body can break them down relatively quickly, reducing the risk of long-term accumulation.
In sports, they emerged as an alternative to anabolic steroids because they were initially beyond the reach of doping tests.
TOP Peptides Discussed in the Fitness Community
Peptides for Recovery and Healing:
BPC-157 – the most widely discussed peptide of all. A synthetic 15-amino acid peptide derived from a protein found in gastric juice. Unlike most peptides, it is stable in gastric juice for over 24 hours, allowing it to be effective even when taken orally. It became a cult product in the US after Joe Rogan and Andrew Huberman talked about it on their podcasts. It is also available in the form of an arginine salt (BPC-157 arginate), which offers potentially better absorption.
TB-500 (Thymosin Beta-4) – a 43-amino acid peptide naturally occurring in the body. It promotes the migration of cells to the site of an injury and the formation of new blood vessels.
TB-4 Fragment (Ac-SDKP) – a shorter, 4-amino acid fragment of TB-500, also available in an oral form (unlike full-length TB-500).
KPV – a tripeptide (3 amino acids) with significant anti-inflammatory effects, used for intestinal inflammation and skin problems.
For Growth Hormone and Muscle Building:
MK-677 (Ibutamoren) – not a peptide, but a growth hormone secretagogue (a small molecule). It stimulates the release of the body's own GH and IGF-1. Popular because it is available in pill form.
IGF-1 (Insulin-like Growth Factor-1) – directly supports muscle growth. IGF-1 DES is often injected straight into the trained muscle for a localized effect.
For Skin and Anti-Aging:
GHK-Cu (Copper Tripeptide-1) – a tripeptide complexed with copper that occurs naturally in the body (levels drop from 200 ng/ml at age 20 to 80 ng/ml at age 60). It is widely used in cosmetics for skin regeneration, wound healing, and anti-aging effects. The FDA permits its topical use (creams, serums) but has placed it in Category 2 for injectable use.
Peptides for Weight Loss
GLP-1 Agonists:
Semaglutide (Ozempic, Wegovy) – FDA-approved, 15% weight loss over 68 weeks.
Tirzepatide (Mounjaro, Zepbound) – a dual GIP/GLP-1 agonist, 22.5% weight loss over 72 weeks.
Orforglipron – the first oral GLP-1 agonist (pills), 12.4% weight loss over 72 weeks at a dose of 36 mg per day.
5-amino-1MQ – blocks the NNMT enzyme, increases metabolism. Available in capsules, though human data is lacking.
The Critical Question: Why Do Most Peptides Not Work Orally?
Here comes the crucial physiological fact that many sellers "forget" to mention: Most peptides do not survive the digestive process.
When swallowing a peptide:
Stomach acid (pH 1-3) – breaks down peptide bonds.
Enzymatic digestion – pepsin, trypsin, and chymotrypsin further fragment the peptides.
Intestinal barrier – even if a peptide survives, only small molecules pass into the blood.
Exceptions That Work Orally:
BPC-157 (arginine salt) – utilizes the peptide's natural stability in gastric juice; the arginine form improves absorption. Human pharmacokinetic studies are currently lacking, but it has demonstrated efficacy in animal models even when administered orally.
TB-4 Fragment (Ac-SDKP) – a smaller fragment of TB-500 that retains the beneficial properties of the original molecule. Due to its smaller size, it has significantly better oral bioavailability than full TB-500.
GLP-1 Agonists – specially stabilized, but still only have ~1% bioavailability (how much of the substance actually enters the bloodstream).
KPV – utilizes the PepT1 transporter in the gut.
5-amino-1MQ – a small molecule with good oral bioavailability.
MK-677 – not a peptide, but a small molecule.
Forms of Administration in Practice
Subcutaneous injection (under the skin) – the most common, 90-100% bioavailability.
Used for: BPC-157, TB-500, GLP-1 agonists, GHRP.
Intramuscular injection (into the muscle) – faster absorption.
Used for: IGF-1 DES (often directly into the trained muscle).
Oral capsules – only for stable peptides/molecules.
Works for: BPC-157 (arginine salt), TB-4 Fragment, 5-amino-1MQ, MK-677, KPV.
Does NOT work for: TB-500 (full molecule), IGF-1 (they are broken down during digestion).
Buccal/Sublingual administration (dissolvable tablets, oral strips) – a newer trend in peptide delivery. A tablet or strip is placed in the mouth (under the tongue or against the cheek) and dissolves over 5-15 minutes, allowing peptides to absorb directly through the highly vascularized oral mucosa into the bloodstream. The advantage is bypassing both stomach acid and first-pass metabolism in the liver.
This method is primarily used for BPC-157 and the combination of BPC-157 + TB-500.
Conventional buccal administration achieves only 1-2% bioavailability for peptides, but modern formulations with absorption enhancers (e.g., SNAC) and nanoparticles improve these figures.
How Peptides Function in the Human Body
Receptor Binding and Cellular Signaling
Peptides operate on a "lock and key" principle. Each peptide has a specific structure that allows it to bind to a corresponding receptor on the cell surface, triggering a cascade of biochemical reactions.
Example (BPC-157): Upon entering the body, it binds to cells in the tendons and ligaments, stimulating collagen production and the formation of new blood vessels (angiogenesis). The result is significantly accelerated healing.
Impact on Hormonal and Metabolic Processes
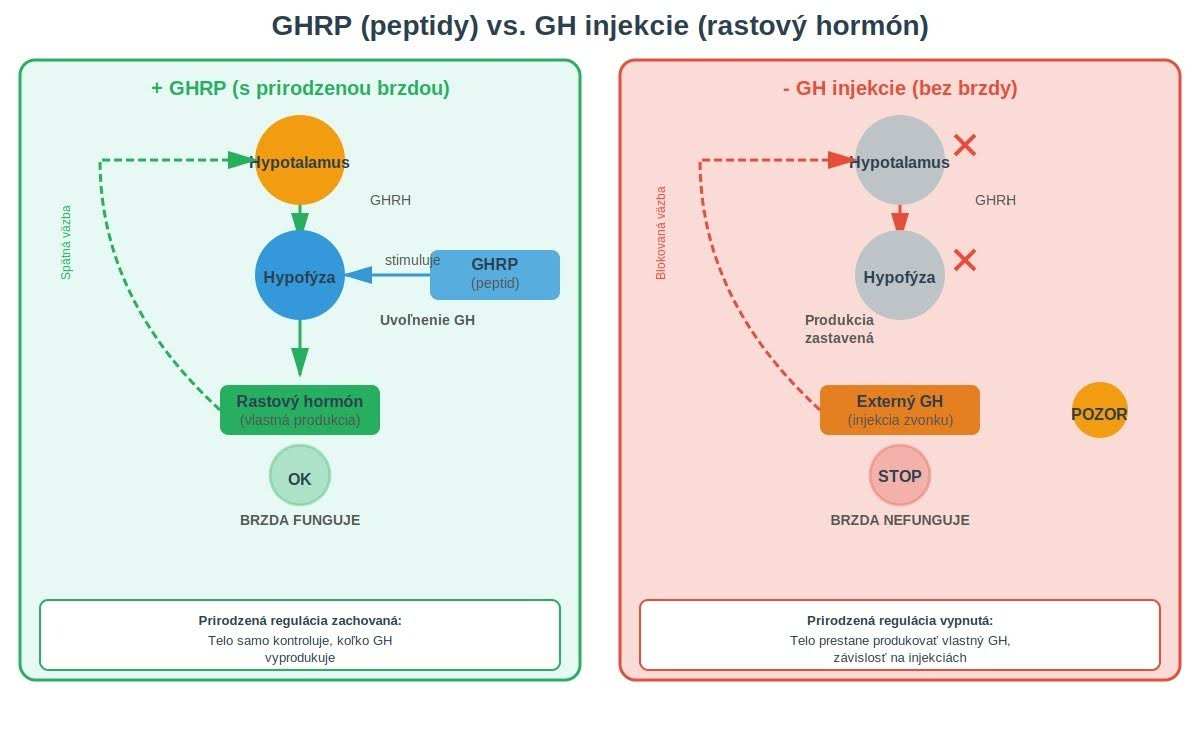
Growth hormone (GH) is naturally released from the pituitary gland. However, the body has a built-in "brake": once it detects sufficient levels of growth hormone, it halts further production.
GHRPs (Growth Hormone Releasing Peptides), such as GHRP-6, GHRP-2, or ipamorelin, act as the "key" that unlocks this natural system. When these are used, the body begins releasing its own growth hormone—but only up to a certain threshold. Once that level is reached, production automatically stops.
The Crucial Difference:
Direct GH Injections: The natural "brake" is bypassed or disabled, causing the body to stop producing its own natural hormone (shutdown).
GHRPs: The body maintains its ability to self-regulate production, which results in a lower risk of side effects.
Created using Claude AI (Anthropic)
Why the Effect Depends on the Type of Peptide
Not all peptides act in the same way. GHRP-6 stimulates the release of growth hormone but also significantly increases appetite, which is problematic for those trying to lose weight. Ipamorelin has a similar effect on growth hormone but does not affect appetite to the same extent. BPC-157 does not affect growth hormone at all; instead, it directly stimulates angiogenesis—the formation of new blood vessels in damaged tissue.
Effects of Peptides According to Scientific Studies
Tissue Regeneration and Healing Studies on rodents have shown impressive results. When scientists intentionally severed the Achilles tendons of rats and subsequently administered BPC-157, healing occurred significantly faster compared to the control group. In another study, rats with damaged thigh muscles that received BPC-157 restored full muscle function within 14 days.
The Mechanism:
Stimulation of angiogenesis (formation of new blood vessels)
Activation of fibroblasts (cells that produce collagen)
Important Notice: Almost all of this data comes from animal studies. Human clinical trials are lacking. A 2024 systematic review stated: "Currently, there are no published clinical trials in humans evaluating BPC-157 for orthopedic use."
Peptides and Weight Loss – What Works
GLP-1 agonists have proven efficacy:
Semaglutide: 15% weight loss over 68 weeks (STEP 1 study, NEJM 2021)
Tirzepatide: 22.5% weight loss over 72 weeks (SURMOUNT-1 study, NEJM)
Orforglipron: 12.4% weight loss over 72 weeks (ATTAIN-1 study, NEJM 2025)
Important: These medications require a medical prescription and regular check-ups. They are intended for obesity (BMI ≥30) or overweight (BMI ≥27) individuals with accompanying health problems.
Other Weight Loss Peptides:
AOD-9604 – failed in human clinical trials (2015).
5-amino-1MQ – promising preclinical data in mice; human studies are lacking.
Metabolism and Body Composition
AOD-9604 is a small fragment of the growth hormone molecule—specifically the end (C-terminus) responsible for fat burning. Manufacturers market it with the claim that it can aid weight loss without affecting blood sugar levels.
In experiments on rats, it worked exceptionally well—burning fat 12 times more effectively than the full growth hormone molecule. The problem is that rats have specific beta-3 adrenergic receptors in their bodies, which we humans possess in significantly smaller quantities.
The Result? In a 2015 press release, Metabolic Pharmaceuticals, the company that tested the peptide in human clinical trials, stated: "AOD-9604 did not result in clinically significant weight loss in the tested population."
Peptides and Weight Loss – What the Research Confirms
GLP-1 Agonists: The Only Peptides with Proven Efficacy GLP-1 (glucagon-like peptide-1) agonists are polypeptide hormones that mimic the action of the natural hormone GLP-1. Originally developed to treat type 2 diabetes, they have demonstrated a significant impact on weight reduction.
How they work:
Slowing gastric emptying → longer-lasting satiety
Reducing appetite by acting on the brain
Improving insulin sensitivity
Lowering blood glucose levels
First Generation: Semaglutide
Semaglutide (Ozempic, Wegovy) was FDA-approved for weight loss in 2021. The STEP 1 study, published in the New England Journal of Medicine (2021), showed:
An average of 15% weight loss over 68 weeks
Application: Once-weekly subcutaneous injection
Dosage: Gradual increase from 0.25 mg to 2.4 mg per week
Second Generation: Tirzepatide (Dual Agonist)
Tirzepatide (Mounjaro, Zepbound) is the first drug of its kind—it simultaneously activates both GIP and GLP-1 receptors, leading to more pronounced effects.
FDA Approvals:
May 2022: Type 2 diabetes
November 2023: Chronic weight management
Results from the SURMOUNT-1 study (NEJM):
At the highest dose (15 mg): an average of 22.5% weight loss over 72 weeks (equivalent to an average loss of 21.8 kg)
89–91% of participants achieved at least a 5% weight loss
50–57% of participants lost more than 20% of their weight
Application: Once-weekly subcutaneous injection
Third Generation: Orforglipron (First Oral) Orforglipron is a breakthrough—the first next-generation oral GLP-1 agonist. Unlike injectable medications, it is a small molecule (not a peptide) taken in pill form.
Results from the ATTAIN-1 study (NEJM, September 2025):
At a dose of 36 mg daily: 12.4% weight loss over 72 weeks
Application: Daily pills
Important Warnings for GLP-1 Agonists
Intended for obesity (BMI ≥ 30)
Or overweight (BMI ≥ 27) with associated health problems (diabetes, hypertension)
Regular medical check-ups are essential
Side Effects:
Common: Nausea, vomiting, diarrhea (usually improve after a few weeks)
Uncommon: Gallstones, pancreatitis
Controversial: Possible loss of muscle mass (up to 25–40% of lost weight may be muscle)
Warning: Many people obtain tirzepatide or semaglutide from illegal sources (online pharmacies, the black market). This is extremely dangerous due to uncertain quality and purity, incorrect dosing, lack of medical supervision, and the risk of counterfeit products.

Risks and Side Effects of Peptides
Observed Short-Term Reactions
GHRP-6 increases cortisol and prolactin levels. While a temporary spike in cortisol is not a long-term issue, elevated prolactin can lead to decreased libido and erectile dysfunction in men. Hexarelin, the most potent of all growth hormone-releasing peptides, triggers the most significant increase in cortisol and prolactin among all GHRPs.
Other reported reactions:
Nausea and dizziness (especially at higher doses)
Water retention and swelling (edema)
Pain at the injection site
Increased appetite (specifically with GHRP-6 and ghrelin analogs)
Potential Long-Term Risks
Most peptides have never been tested in long-term human studies. Theoretical risks include:
Angiogenesis and Tumors: BPC-157 promotes the formation of new blood vessels, which aids healing - however, tumors utilize the same mechanism to grow and spread. Paradoxically, some animal studies have shown that BPC-157 can actually block a substance that tumors produce to create blood vessels (VEGF). Some research even suggests it may inhibit the growth of certain types of tumors. Current data is unclear and contradictory; safety regarding cancer has not been verified in humans.
Insulin Resistance: Growth hormone and the peptides that release it can cause insulin resistance by increasing free fatty acids in the blood. Long-term insulin resistance is a precursor to type 2 diabetes.
Receptor Desensitization: With continuous, long-term use of Hexarelin, its effectiveness drops by up to 75% - the body adapts by reducing the sensitivity of receptors to the constant signal.
Why Self-Administration Is Problematic
Peptides purchased on the internet originate predominantly from Chinese laboratories with minimal quality control. Statistics show that 26% of peptides contain no active substance at all, and dozens of other products are significantly underdosed (containing only 30–70% of the declared amount). Positive anecdotal experiences may simply reflect the minority who received a high-quality product.
Real-life case: In 2015, Gavin Burns Smith was sentenced to 3 years in prison and fined $2.1 million. He sold peptides as "research chemicals" intended strictly for laboratory use, yet simultaneously provided customers with advice on how to dose them for human consumption.
A similar problem exists with prohormones and designer steroids. Read more about this issue in the article: Prohormones and Designer Steroids: Effects, Risks, and What Research Says. |
When purchasing peptides, it is important to verify:
COA (Certificate of Analysis):
Proves the product contains exactly what the label claims.
Verifies purity (ideally ≥98%).
Detects contaminants.
Confirms the identity of the substance (via HPLC, mass spectrometry).
Certifications:
GMP (Good Manufacturing Practice)
ISO certificates
Manufacturer Transparency:
Publicly available test results.
Origin of raw materials.
Peptides, Sports, and Regulation
Misuse of Peptides in Sports
Peptides gained popularity in sports because, until recently, they were not included in standard doping tests. GHRPs were not detectable by the standard methods used to identify injections of exogenous growth hormone.
Professional athletes have used them primarily for the following reasons:
Accelerated recovery after injuries (BPC-157, TB-500).
Increased endurance (by promoting the production of red blood cells, which carry oxygen to the muscles).
Protection of connective tissue during high training loads.
Bypassing doping controls (standard tests failed to detect them for years).
Why Some Peptides Are Prohibited
The World Anti-Doping Agency (WADA) classifies a substance as prohibited if it meets at least two of three established criteria. All GHRPs (GHRP-6, GHRP-2, ipamorelin, hexarelin) and GHRH analogs (CJC-1295, tesamorelin) are banned without exception. They are listed under Category S2 (Peptide Hormones, Growth Factors) and are prohibited at all times—both in training and during competition.

Statements from WADA and Regulatory Bodies
In March 2020, the U.S. Anti-Doping Agency (USADA) issued a warning regarding BPC-157. Key points:
BPC-157 is an experimental drug not approved for human use
There is no established safe or effective dose for humans
Long-term risks are unknown
Although not explicitly banned, it falls under the category of "experimental substances"
💡 WADA continuously updates its Prohibited List. Since 2016, testing has been expanded to include the detection of GHRP peptides using mass spectrometry - a laboratory method that can precisely identify which substances are present in the urine or blood and in what amounts. |
Anecdotal Experience vs. Clinical Data
Why Internet Experiences Are Not Evidence
Hundreds of enthusiastic reviews can be found on forums and discussion groups. Why can't these experiences be considered relevant evidence?
Placebo effect: In studies with BPC-157, control groups receiving a placebo often reported a 30-40% improvement in symptoms. The placebo effect is particularly strong when it comes to joint pain.
Influence of other factors: A person who starts taking a peptide often simultaneously changes their training, diet, protein intake, or sleep schedule. The improvement could be the result of any of these changes, not the peptide itself.
Biased feedback: People who express their opinions on internet forums are primarily those who were satisfied with the product.
Fake products: If 26% of products contain no active substance at all and many others are underdosed, positive experiences may only reflect those who actually received a high-quality product.
The Difference Between an Anecdote and a Clinical
Trial A clinical trial has strict criteria:
Randomization: Participants are randomly assigned to groups.
Control group: Comparison with a placebo or standard treatment.
Double-blindness: Neither the participant nor the researcher knows who is receiving the active substance.
Statistical analysis: The results must be statistically significant (p < 0.05).
Replication: The results should be confirmed by independent studies.
Anecdotal evidence meets none of these criteria.
Limitations of Current Research
Current peptide research has several limitations:
Animal models: A rat with a severed Achilles tendon is not the same as an injured professional footballer. Metabolism, receptors, and reactions to substances differ.
Absence of long-term data: Some studies lasted only 14-90 days. But what happens after a year of continuous use?
Conflict of interest: Most published studies on BPC-157 originate from a single research team in Croatia, with the lead author listed on the patent for BPC-157.
Small sample sizes: A typical study has only 8-16 participants, which is statistically insufficient.
Research Peptides and the Current State of Science
What Current Studies Are Investigating
Ongoing clinical trials are focusing on:
BPC-157 for ulcerative colitis: Testing the administration of the peptide rectally for chronic intestinal inflammation. The study is in Phase 2, which means efficacy and safety are being verified on a larger group of patients.
Tesamorelin for visceral obesity: A peptide approved by the U.S. FDA (Food and Drug Administration) for the treatment of abnormal fat accumulation in the abdominal area in patients with HIV. Tesamorelin stimulates the release of growth hormone, which helps reduce deep belly fat.
Semaglutide for weight loss: A drug originally developed for diabetes that has demonstrated a significant effect on weight reduction in clinical trials.
Why Peptides Are Labeled as Research Substances
A substance is labeled as a "research chemical" for one of the following reasons:
It has not passed Phase 1-3 clinical trials
It has not been approved by any medical agency (FDA, EMA)
There is no safety data regarding long-term use in humans
💡 Companies selling these substances protect themselves with the legal disclaimer "for laboratory research only, not for human consumption." In practice, however, it is clear that the target audience consists of athletes and bodybuilders. |
The Future of Peptides in Medicine
Peptide therapy has significant potential in medicine. Proven applications include:
Insulin: a peptide hormone for diabetes (used since 1922).
GLP-1 agonists: treatment for diabetes and obesity.
The key difference: all these peptides have undergone dozens of studies, have clearly defined indications, and are prescribed under medical supervision.
Why It Is Important to Understand the Risks
Using unapproved peptides carries specific risks that go beyond the common side effects of medications:
Unknown purity and content: Without quality control, we do not know if the product contains contaminants. It is also uncertain whether it actually contains the declared substance and, if so, in what quantity. For example, analyses of black-market peptides have shown that up to 26% of samples contain no active substance at all.
Absence of dosing protocols: Dosing is based on forum discussions and anecdotal recommendations, not on pharmacological data from clinical trials. An effective dose for a rat of 10 mcg/kg does not automatically mean that the dose for a 70 kg human is 700 mcg.
Absence of long-term data: Some studies lasted only 14-90 days. However, side effects can manifest even years later.
Legal consequences: In many countries, possession of these substances without a prescription is illegal. Athletes risk a lifetime ban from competition.
The Importance of Professional Supervision and Regulation
Medical supervision when using any biologically active substances is not bureaucracy, but a necessity:
Laboratory monitoring: Regular checks of hormone levels (IGF-1, TSH, cortisol, prolactin), glucose, lipid profiles, and liver enzymes can detect problems before they become serious.
Individualization of treatment: People react to peptides differently. A person with low growth hormone may benefit from GHRPs, whereas someone with normal levels might only experience side effects.
Detection of interactions: Peptides affect the metabolism of other drugs. For example, GHRPs can worsen the efficacy of antidiabetic medications by increasing insulin resistance.
Legal protection: In the event of adverse side effects from illegally purchased peptides, the consumer has no legal protection or possibility of compensation.
Education as Prevention Against Misuse
Scientific data state the following facts about peptides:
They do not work as commonly claimed (AOD-9604).
They only work under specific conditions (GHRPs only with exercise).
They have side effects that outweigh the benefits (e.g., hexarelin significantly increases cortisol and prolactin levels).
They have never been tested on humans in clinical trials (BPC-157).
Real benefits from a scientific perspective:
Collagen peptides: proven improvement in skin appearance and joint health at a daily dose of 10-15 g.
Creatine: technically a tripeptide, the most thoroughly researched performance-enhancing supplement.
Approved medications: GLP-1 agonists for obesity and diabetes.
Safe Alternatives for Supporting Growth and Recovery
If you are looking for natural support without the risks associated with experimental peptides, there are proven supplements based on natural ingredients. You can find them in our e-shop at aminoxy.com.
To support testosterone and hormonal balance:
T-1000 TESTO EXTREME – a comprehensive formula containing Tribulus Terrestris (900 mg), Long Jack P.E., 20-Hydroxyecdysterone, and an estrogen-inhibiting complex with Luteolin and Apigenin. Unlike peptides, it works with the body's natural mechanisms without suppressing its own hormonal production.
To support growth and recovery:
SST-1: GH – a supplement supporting the natural production of growth hormone during sleep using Mucuna Pruriens (L-DOPA) and anterior pituitary peptides. It works by stimulating your own pituitary gland, not by supplying synthetic hormones.
SST-1: IGF – contains N2P-GF Whey Protein Isolate with natural growth factors similar to IGF-1, protected by liposomal technology for maximum absorption.
For advanced research (for professional use only):
MYO-STACK – research material containing 5-Alpha-Hydroxy Laxogenin, Turkesterone, and Ajuga Turkestanica extract. Intended exclusively for laboratory purposes, not for human consumption.
The key difference between these products and black-market peptides:
Legally available
Laboratory tested (COA certificates)
GMP certified
Clear dosing and safety information
Legal consumer protection
See more from our Testosterone support category.
Peptides represent an interesting area of research with significant potential in medicine. But as we have shown - most of those sold on the black market lack sufficient human data, carry unknown risks, and often do not even contain what is on the label. Education about their true effects and limitations is the best prevention against their misuse.
Read also:
The Hidden Face of Nutritional Supplements: What Are We Really Consuming?
How to Check Your Testosterone Levels: A Guide for Hormonal Detectives.
Sources
Brainum, J. "BPC 157: Miracle Cure for Muscle and Joint Injuries or Just Hype?" – Applied Metabolics Newsletter, február 2022
Brainum, J. "Growth Hormone-Releasing Peptides: Do they work?" – Applied Metabolics, jún 2017
Brainum, J. "A Growth Hormone-Releasing Supplement That Works?" – Applied Metabolics Newsletter, december 2021
Brainum, J. "Are Hydrolyzed Collagen Peptides a Useful Supplement?" – Applied Metabolics Newsletter, apríl 2022
Sikiric, P., et al. "Stable gastric pentadecapeptide BPC 157: Novel therapy in gastrointestinal tract" – Journal of Physiology - Paris, 97(3-4), 1993
Veljaca, M., et al. "Digestion of h-EGF, h-TGF alpha, and BPC-15 in human gastric juice" – Gastroenterology, 108(4), A761, 1995
Sikiric, P., et al. "Pentadecapeptide BPC 157 and the central nervous system" – Neural Regeneration Research, 17(3), 482-487, 2022
Heffernan, M., et al. "The effects of human GH and its lipolytic fragment (AOD-9604) on lipid metabolism" – Journal of Endocrinology, 168(1), 2001
Geyer, H., Parr, M.K., et al. "Analysis of non-hormonal nutritional supplements for anabolic-androgenic steroids - results of an international study" – International Journal of Sports Medicine, 25(2), 2004
Wilding, J.P.H., et al. "Once-Weekly Semaglutide in Adults with Overweight or Obesity" – New England Journal of Medicine, 384(11), 989-1002, 2021
Jastreboff, A.M., et al. "Tirzepatide Once Weekly for the Treatment of Obesity" – New England Journal of Medicine, 387(3), 205-216, 2022
Rosenstock, J., et al. "Once-Daily Oral Orforglipron for Adults with Obesity" – New England Journal of Medicine, 393(12), 1116-1130, 2025
Liu, J., et al. "Nicotinamide N-methyltransferase knockdown protects against diet-induced obesity" – Nature, 508(7496), 258-262, 2014
Xiao, B., et al. "Orally Targeted Delivery of Tripeptide KPV via Hyaluronic Acid-Functionalized Nanoparticles Efficiently Alleviates Ulcerative Colitis" – Biomacromolecules, 18(6), 1747-1758, 2017
Pather, I., et al. "Delivery of bioactive peptides and proteins across oral (buccal) mucosa" – Current Pharmaceutical Biotechnology, 2(2), 175-186, 2001
Hua, S. "Advances in Nanoparticulate Drug Delivery Approaches for Sublingual and Buccal Administration" – Frontiers in Pharmacology, 10:1328, 2019
"Overcoming Oral Cavity Barriers for Peptide Delivery Using Advanced Pharmaceutical Techniques and Nano-Formulation Platforms" – Biomedicines, 13(11), 2735, 2025
Goldstein, A.L., et al. "Thymosin β4: A multi-functional regenerative peptide" – Annals of the New York Academy of Sciences, 1194(1), 179-189, 2010
Kassem, K.M., et al. "Tβ4-Ac-SDKP pathway: Any relevance for the cardiovascular system?" – Canadian Journal of Physiology and Pharmacology, 97(7), 589-599, 2019
Pickart, L., Margolina, A. "Regenerative and Protective Actions of the GHK-Cu Peptide in the Light of the New Gene Data" – International Journal of Molecular Sciences, 19(7), 1987, 2018
"Emerging Use of BPC-157 in Orthopaedic Sports Medicine: A Systematic Review" – PMC (PubMed Central), 2024
World Anti-Doping Agency (WADA). "Prohibited List 2024" – https://www.wada-ama.org
U.S. Anti-Doping Agency (USADA). "BPC-157 Peptide Warning" – Press Release, marec 2020
U.S. Food and Drug Administration. "Bulk Drug Substances That May Present Significant Safety Risks - Category 2" – FDA.gov, september 2023
PubMed Central – National Library of Medicine – https://pubmed.ncbi.nlm.nih.gov