A trend is spreading across fitness forums and social media: capsules with natural-sounding names that promise up to 5 kg of lean muscle per month without side effects. In the bodybuilding community, they are referred to as "category 3 steroids" — substances positioned somewhere between natural supplements and classic steroids. No injections, no doctor's prescriptions, no legal troubles. Sounds like the perfect solution, right?
However, the reality is different. A 2017 study published in the journal JAMA tested 44 products. Only 52% contained what was on the label. Another 39% contained a completely different unapproved substance, and 9% contained nothing at all.
What are SARMs
Definition of SARMs (Selective Androgen Receptor Modulators)
SARMs stands for Selective Androgen Receptor Modulators. These are synthetic chemicals created in laboratories designed to mimic the effects of testosterone, but theoretically only in specific parts of the body.
To understand this, we must first explain what androgen receptors are. Imagine them as locks in cells that react to keys — hormones like testosterone. When testosterone binds to these receptors, the cell receives a signal: "Start building muscle," "Increase bone density," or "Activate sebaceous glands in the skin."
Receptors are scattered throughout the entire body — in muscles, bones, the prostate, hair follicles, and skin. This is why testosterone (or anabolic steroids) acts everywhere at once: muscle mass increases, but at the same time, the prostate can enlarge, hair might fall out, or acne may develop.
SARMs were supposed to be different — they were designed to bind only to receptors in muscles and bones while avoiding other tissues.
The most well-known SARMs and similar substances:
Ostarine (MK-2866) – the most researched, originally tested on patients with muscle wasting. In bodybuilding, it is used to preserve muscle during a diet.
Ligandrol (LGD-4033) – developed to treat muscular dystrophy, popular in gyms for gaining mass (bulking).
Testolone (RAD-140) – often referred to as the "strongest SARM," it is popular in bodybuilding, with users reporting a significant increase in strength.
Andarine (S-4) – tested for osteoporosis, used for muscle definition and cutting.
S23 – a potent SARM used for definition, which severely suppresses natural testosterone production.
YK-11 – a specific substance that blocks myostatin (a protein that limits muscle growth).
MK-677 (Ibutamoren) – not a SARM, but a growth hormone secretagogue (stimulator). It is used for recovery and growth.
MK-777 (Acetamoren) – marketed as an improved analog of MK-677. There are no published human clinical trials.
SR9009/SR9011 – not SARMs, but compounds that affect metabolism and circadian rhythms.
Cardarine (GW-501516) – not a SARM, but a compound that increases endurance and fat burning.
Most of these substances have never been approved for human use and are banned by WADA (World Anti-Doping Agency). Other substances like RAD-150, ACP-105, or GW-0742 appear on the black market, but there are no published human clinical trials or safety data available for them.
Why SARMs were developed
In the 1990s, pharmaceutical companies were looking for treatments for severe health conditions associated with muscle wasting:
Sarcopenia – muscle loss associated with aging.
Cachexia – a complex metabolic syndrome characterized by extreme weight loss, particularly muscle wasting, commonly seen in cancer or AIDS patients.
Muscular dystrophy
Osteoporosis
The problem with classic therapy (testosterone, anabolic steroids) was obvious: yes, they promote muscle growth, but simultaneously cause prostate enlargement, acne, hair loss, or virilization. Virilization means the development of male physical characteristics in women — such as a deepening of the voice, increased body hair growth, or changes in the menstrual cycle.
The goal of developing SARMs was to find a substance that would:
Promote muscle and bone growth
Not affect the prostate
Not cause masculinizing effects
The result? Dozens of molecules passed laboratory testing, and some advanced to clinical trials. However, not a single one was ever approved as a medicine.
The pharmaceutical industry eventually stepped back from SARMs, but the substances found their way onto the black market and into commercial gyms. Today, in the bodybuilding and fitness community, they are viewed as a compromise between natural supplements and anabolic steroids — offering some of the benefits of steroids with theoretically lower risks. However, this assumption is misleading, which we will discuss later.

The Difference Between SARMs and Anabolic Steroids
Although SARMs are often compared to steroids, there are important differences between them.
Chemical structure: Steroids have a molecule derived from testosterone — four fused carbon rings. SARMs have a different chemical structure; they are not steroids in the true sense of the word.
Form of administration: Most steroids are administered via injection. SARMs are available in tablets, capsules, or liquid form.
Aromatization: Steroids can convert into estrogen (the female hormone) in the body. SARMs do not convert into estrogen.
Selectivity: Steroids act in all tissues containing androgen receptors. SARMs were designed to be selective — theoretically acting only in muscles and bones.
Despite these differences, SARMs and steroids share one fundamental problem: both groups of substances suppress natural testosterone production and carry health risks.
We wrote in more detail about the issue of steroids and prohormones in the article Prohormones and Designer Steroids: Effects, Risks, and What the Research Says.
How SARMs Act in the Human Body
Androgen Receptors and Their Role
An androgen receptor is a protein found inside cells. Its role is simple: to wait for a signal from hormones (androgens) and subsequently trigger specific processes within the cell.
How it works step-by-step:
Testosterone (or another androgen) enters the cell.
It binds to the androgen receptor.
This complex moves into the cell nucleus.
In the nucleus, it influences genes responsible for protein production.
The cell begins producing new proteins — the building blocks of muscle.
This process takes place in many tissues simultaneously:
In muscles — it promotes growth and recovery.
In bones — it increases density and strength.
In the prostate — it stimulates growth (a problem in case of overactivation).
In hair follicles — it can lead to hair loss.
In the skin's sebaceous glands — it increases sebum production (acne).
SARMs bind to these exact same receptors. The difference lies in how strongly and where they bind.
Selectivity — Theory vs. Reality
The main idea behind SARMs was: "What if we created a substance that activates receptors only in muscles and bones, but avoids the prostate and skin?"
Problem No. 1: The receptor is the same everywhere An androgen receptor in a muscle looks exactly the same as a receptor in the prostate. The SARM molecule sees no difference — it is still the exact same "lock."
Problem No. 2: Selectivity is only relative Studies show that SARMs do indeed possess a certain selectivity — they have a stronger effect in muscles than in the prostate. However, this comparison only holds true at low doses. At higher doses, meaning the kind used in the real world, this selectivity is lost.
A study on Ostarine published in the journal Clinical Endocrinology tested the effects on 120 volunteers over 12 weeks. The results showed not only an increase in muscle mass, but simultaneously a significant:
Decrease in HDL cholesterol ("good" cholesterol)
Suppression of natural testosterone production
Increase in liver enzymes in 18% of participants
Why "Selectivity" Does Not Mean Safety
Marketing surrounding SARMs claims: "All the benefits of steroids, none of the side effects." The reality is different.
1. Suppression of natural testosterone production
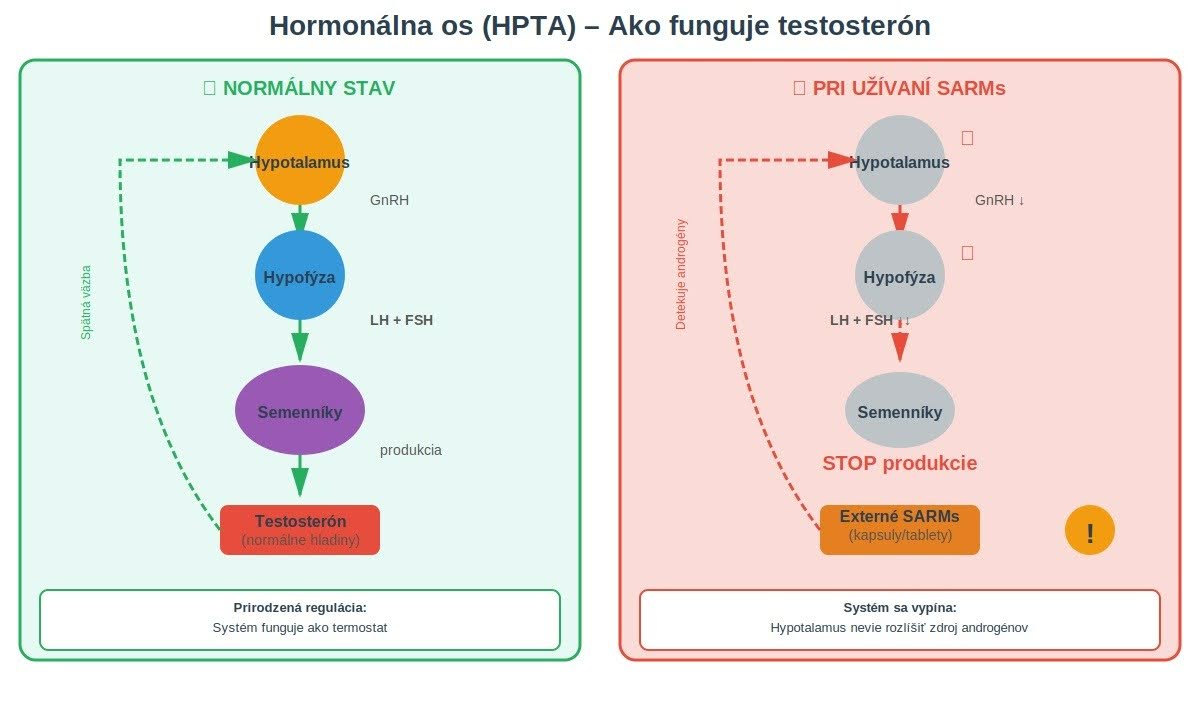
The body has a feedback loop system. The hypothalamus continuously measures the level of androgens in the blood. When it detects there are enough of them, it sends a signal: "Stop testosterone production."
The problem? The hypothalamus cannot distinguish whether the androgen comes from the testes or from a SARM capsule. The result is the same: natural testosterone production drops.
2. Impact on cholesterol
All tested SARMs lower HDL cholesterol and increase LDL cholesterol. The higher the dose, the greater the drop in HDL. This effect increases the risk of cardiovascular disease.
3. Strain on the liver
Oral SARMs (in tablet or capsule form) pass through the liver, where they can cause an increase in liver enzyme levels (ALT, AST). These enzymes are markers of liver damage — their elevated presence in the blood means that liver cells are stressed or dying and releasing their contents into the bloodstream.
💡 The selectivity of SARMs is only a relative advantage compared to steroids – it does not mean that they are safe or without side effects. |
Effects of SARMs According to Scientific Studies
Effects Observed in Clinical Studies
Most data on SARMs comes from short-term clinical trials lasting 8–16 weeks. No long-term studies have been published.
Ostarine (MK-2866):
A study published in the Journal of Clinical Oncology (2011) tested Ostarine on 159 patients with cancer cachexia for 16 weeks.
Results:
Increase in muscle mass: 1.5 kg at a dose of 3 mg/day
Improvement in physical function
But: A 23–43% decrease in testosterone and a 17–27% reduction in HDL cholesterol
Ligandrol (LGD-4033):
A study from The Journals of Gerontology (2013) tested Ligandrol on 76 healthy men for 21 days.
Results at a dose of 1.0 mg/day:
Increase in muscle mass: 1.21 kg
Increase in lower limb strength
But: A 55% decrease in testosterone
Testolone (RAD-140):
There are no published human clinical trial results for RAD-140. Available data comes exclusively from animal testing.
Short-Term Physiological Reactions
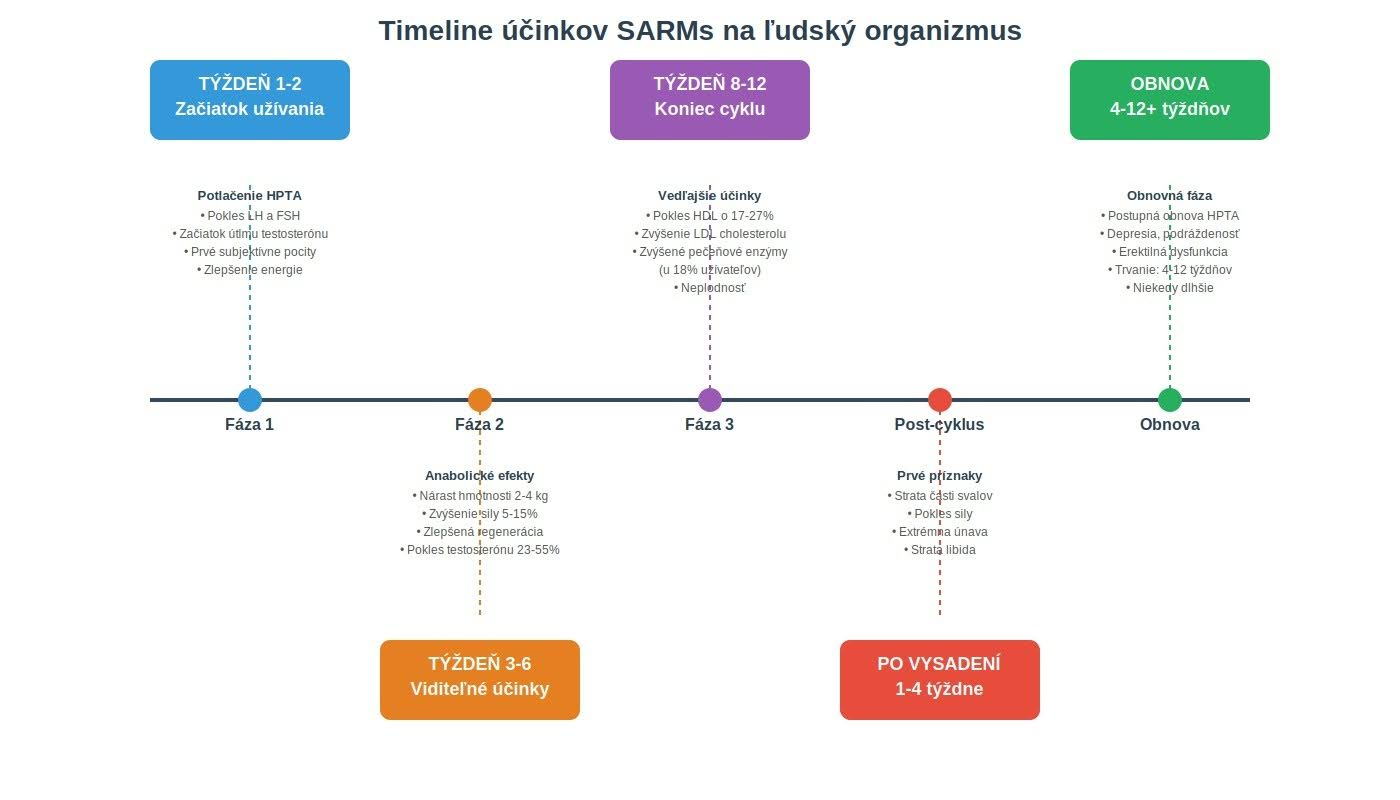
When using SARMs, weight gain (2–4 kg), increased strength (5–15%), and subjective energy improvements typically occur within the first few weeks. Concurrently, however, the suppression of natural testosterone production and negative shifts in the lipid profile begin.
After discontinuing use, individuals often experience a loss of a portion of the muscle mass gained during the cycle, accompanied by symptoms of low testosterone. Natural hormone recovery takes an average of 4–12 weeks.
Created using Claude AI (Anthropic)
What We Don't Know Yet — Research Limits
Most published clinical studies date back to the years 2011–2013. This is also the period when pharmaceutical companies halted further development of SARMs due to an unfavorable risk-benefit ratio. Since 2018, the only publications appearing are meta-analyses, systematic reviews, or case reports of patients with serious side effects.
Main unresolved questions:
Long-term safety: Studies lasted for a maximum of 12–16 weeks.
Real-world doses: In practice, real-world doses are 10 to 30 times higher than those used in clinical studies.
Missing demographic data: Data regarding the effects on women and young people is completely lacking.
Potential Risks and Side Effects
Impact on the hormonal axis (HPTA)
When SARMs enter the body, the hypothalamus detects the androgen and signals: "We have enough testosterone, stop production." Consequently, its production in the testes is shut down.
Clinical studies consistently show a significant suppression of natural testosterone production across all tested SARMs. The recovery of natural production takes several months on average.
The consequences of suppressing natural testosterone production include:
Extreme fatigue
Depression and irritability
Loss of libido
Erectile dysfunction
Infertility
Created using Claude AI (Anthropic)
Liver, Lipid Profile, and Cardiovascular Risks
Hepatotoxicity (liver damage): Oral SARMs (in tablet form) pass through the liver, where they can cause an increase in liver enzymes (ALT, AST). Cases of acute liver injury are well-documented in medical literature.
Case Report: A case report (a detailed description of a specific patient's case in medical literature) published in the journal Frontiers in Pharmacology (2020) describes a 24-year-old man who used Ligandrol and Ostarine for 8 weeks. This resulted in an ALT increase to 1200 U/L (the normal value is below 40), jaundice, and required hospitalization.
Lipid profile:
All tested SARMs lower HDL cholesterol by an average of 20–40% and increase LDL cholesterol. These changes significantly increase the risk of atherosclerosis and cardiovascular disease.
Risks of Long-Term Use
Since long-term studies do not exist, it remains unknown what diseases SARMs may cause with prolonged use. Furthermore, real-world doses used in practice are often 10 to 30 times higher than those used in clinical trials.
SARMs and Abuse in Sports
Why SARMs are banned by WADA
The World Anti-Doping Agency (WADA) added SARMs to the prohibited list in 2008 under category S1. Anabolic Agents.
SARMs meet all three of WADA's criteria for a ban:
They enhance performance – by promoting muscle growth.
They pose a health risk – by suppressing testosterone and negatively impacting cholesterol.
They violate the spirit of sport – by providing an unfair advantage.
SARMs are prohibited at all times (both in-competition and out-of-competition) for all athletes.
Doping cases and the reality of testing
In 2019, more than 900 positive tests for SARMs were recorded worldwide. The most frequently detected SARMs were:
Ostarine – 45% of cases
Ligandrol – 28% of cases
Testolone – 15% of cases
The contamination problem:
Many athletes claim they inadvertently consumed SARMs through a contaminated dietary supplement. This argument is not entirely unfounded.
A study from JAMA (2017) analyzed 274 dietary supplements:
52% contained one or more SARMs.
Only 41% contained exactly what was stated on the label.
39% contained a different, unapproved substance.
Ethical and Health Consequences
The use of SARMs in sports creates an uneven playing field and undermines fair play. When elite athletes and influencers present SARMs as a "safe alternative," they normalize dangerous behavior and create immense pressure: "Either cheat, or you'll never win." This creates a completely false image of what can actually be achieved naturally.
Myths and Reality Surrounding SARMs
"The Strongest SARM" — Why this is a misleading concept
On the internet, we frequently encounter information ranking the "strongest SARMs," with RAD-140 (Testolone) often taking the top spot. Why is this terminology problematic?
"Strength" is not an exact parameter: The concept of the "strongest SARM" is problematic because strength is not a precisely defined medical metric. What exactly does it mean? Faster muscle growth? Higher incidence of side effects?
Higher efficacy = higher risks: If a certain SARM is biologically "stronger," it likely also exerts a harsher impact on natural testosterone suppression and lipid profiles.
Animal testing data ≠ human reality: Many claims about these compounds rely exclusively on the results of animal testing. However, these results are not directly transferable to humans — the efficacy and safety profile in the human body can be completely different. Human clinical trials are severely lacking for the majority of SARMs on the market.

Experiences vs. Clinical Data
When discussing SARMs, it is important to distinguish between subjective individual SARMs experiences (anecdotes) and scientific data (controlled studies).
How SARMs are used in practice
In commercial gyms, SARMs are utilized for specific goals. The problem is that real-world doses (10–30 mg daily) are 10 to 30 times higher than those used in clinical trials.
Gaining muscle mass (Bulking):
Substances used: Ligandrol, RAD-140, MK-677
What users report: Gains of 3–5 kg in 8–12 weeks
What studies show: 1–2 kg at low doses (1–3 mg/day)
The difference: Most of the real-world gain is water retention, not pure lean muscle.
Definition and fat burning (Cutting):
Substances used: Ostarine, Cardarine, SR9009
What is claimed: Muscle preservation during a diet, increased fat burning
What the data says: Human clinical trials for this specific purpose are completely lacking.
Recovery and growth:
Substance used: MK-677
What it does: Increases growth hormone levels
Side effects: Water retention, increased appetite, fatigue
This means that users are actively experimenting with doses and substance combinations that have never been tested for safety.
Why are subjective experiences unreliable?
1. The placebo effect When a person pays for a product and expects dramatic results, the brain can convince them that they are seeing those results, even if no physiological change has occurred.
2. Unknown product content Many products labeled as "SARMs" contain substances other than what is stated on the label. This means that SARMs experiences shared online are often based on completely different illicit chemical compounds.
3. Missing context When someone writes "I gained 8 kg in 12 weeks," we don't know how much of that weight is water and how much is actual skeletal muscle. We also lack crucial information regarding their blood work panels and what health complications occurred after they discontinued use.
Example of the difference:
Typical SARMs experience on online forums: "Ligandrol is amazing! I gained 10 kg in 8 weeks!"
Clinical study: An average increase of 1.21 kg of lean muscle mass over 3 weeks.
The difference? In the clinical study, actual lean muscle mass (excluding water) was strictly measured, whereas the user's subjective experience refers to overall scale weight gain.
Why internet claims are not proof
Internet claims do not constitute scientific proof because they lack a control group, objective measurement metrics (such as DEXA scans or comprehensive blood work), and are frequently paid reviews driven by commercial interests.
💡 Rely only on published scientific studies in peer-reviewed journals – not on anonymous posts on forums. |
What Current Research Says
Findings from PubMed and scientific databases
When searching for "SARMs" in the PubMed database (as of December 2024), we find more than 1,200 publications. Research consistently shows the same conclusion: while SARMs do work, the risk-benefit ratio is unfavorable.
A systematic review published in Sexual Medicine Reviews (2019) documents frequent side effects, including acute liver injury (such as the case report from Frontiers in Pharmacology, 2020) and cardiovascular complications.
Why SARMs Are Not Approved as Medications
Despite 20 years of research, no SARM compound has been approved by regulatory authorities (such as the FDA in the US or the EMA in Europe) due to an unfavorable risk-benefit ratio. Studies lasted a maximum of 12–16 weeks, which is far too short to assess long-term risks. For conditions like sarcopenia, approved alternatives already exist.
Examples of halted projects:
Ostarine (GTx-024): Development halted in 2013.
Ligandrol (LGD-4033): Development terminated in 2015.
Positions of Physicians and Regulatory Authorities
FDA (USA):
In 2017, the FDA issued an official warning: "SARMs are experimental drugs that have not been approved. Selling them as dietary supplements is illegal. SARMs pose serious health risks, including heart attacks and liver damage."
EMA (Europe):
The EMA has not granted approval to any substance from the SARM group. SARMs are classified as prescription-only medicines.
Endocrine Society:
From their 2019 position statement: "SARMs are not a safe alternative to steroids. The use of these substances without medical supervision is dangerous and is not recommended."
Conclusion — Informed Decision-Making and Prevention
Why it is important to understand the risks
SARMs are not a safe alternative to steroids. They are experimental drugs that:
Suppress natural testosterone production
Negatively affect cholesterol levels
Can damage the liver
Lack long-term safety data
Are not approved for human consumption
The importance of legal and safe alternatives
For those looking for ways to optimize performance, there are proven alternatives:
Creatine and performance:
Creatine Monohydrate – the most thoroughly researched supplement; it increases strength and supports recovery.
Beta-alanine – helps during intense workouts lasting 60–240 seconds.
Proteins and amino acids:
Whey Protein – a fast-absorbing protein ideal for post-workout nutrition.
EAAs – complete essential amino acids for muscle recovery.
Testosterone and hormonal balance support:
T-1000 TESTO EXTREME – a comprehensive formula containing Tribulus terrestris, zinc, and vitamin D3.
EPI CAT – contains epicatechin, which supports anabolic processes.
You can find the full selection in the category: Testosterone Support
For Professional Use and Research
For advanced research on growth hormone and anabolic response (IN VITRO):
MK-777 – an elite GH/IGF-1 research stack with Acetamoren, peptides, and adaptogens, aimed at monitoring muscle growth, recovery, and cellular renewal.
IBUTA MOREN – a sophisticated bio-active matrix with Ibutamoren and GHK-Cu peptides, designed for the analysis of systemic recovery, energy metabolism, and hormonal signaling.
For the protection and regeneration of liver functions (IN VITRO):
LIVER LONGER – a comprehensive hepatoprotective formula with NAC, TUDCA, and GHK-Cu peptides, designed to monitor cellular protection, detoxification, and liver tissue recovery during extreme metabolic stress.
Products in this category are intended exclusively for laboratory and professional purposes – they are not dietary supplements. We test all substances in this category in cooperation with an ecotoxicological center and specialized laboratories. Check out the category: Special Products
Education Instead of Shortcuts
Most people do not utilize even half of their natural potential. Consulting with experts (such as a trainer or a nutritionist) can save you years of searching through ineffective methods.
The reality of results without SARMs:
Natural growth is slower, but it is sustainable:
First year: 5–10 kg of muscle
Second year: 2–5 kg
Third year and beyond: 0.5–2 kg per year
These numbers may seem small, but these are results that last and do not compromise your health.
Read also:
How to determine testosterone levels: A guide for hormonal detectives.
Prohormones and designer steroids: effects, risks, and what research says.
Sources
Dalton J.T., Barnette K.G., Bohl C.E., et al. "The selective androgen receptor modulator GTx-024 (enobosarm) improves lean body mass and physical function in healthy elderly men and postmenopausal women" – Journal of Cachexia, Sarcopenia and Muscle, 2011
Basaria S., Collins L., Dillon E.L., et al. "The safety, pharmacokinetics, and effects of LGD-4033, a novel nonsteroidal oral, selective androgen receptor modulator, in healthy young men" – The Journals of Gerontology: Series A, 2013
Van Wagoner R.M., Eichner A., Bhasin S., Deuster P.A., Eichner D. "Chemical composition and labeling of substances marketed as selective androgen receptor modulators and sold via the internet" – JAMA, 2017
Solomon Z.J., Mirabal J.R., Mazur D.J., Kohn T.P., Lipshultz L.I., Pastuszak A.W. "Selective androgen receptor modulators (SARMs) - current knowledge and clinical applications" – Sexual Medicine Reviews, 2019
Thevis M., Schänzer W. "Detection of SARMs in doping control analysis" – Molecular and Cellular Endocrinology, 2018
Narayanan R., Coss C.C., Dalton J.T. "Development of selective androgen receptor modulators (SARMs)" – Molecular and Cellular Endocrinology, 2018
Gao W., Dalton J.T. "Expanding the therapeutic use of androgens via selective androgen receptor modulators (SARMs)" – Drug Discovery Today, 2007
Bhasin S., Jasuja R. "Selective androgen receptor modulators (SARMs) as function promoting therapies" – Current Opinion in Clinical Nutrition & Metabolic Care, 2009
Kintz P., Ameline A., Gheddar L., Raul J.S. "Testing for SARMs in sport: Experience from laboratory practice" – Drug Testing and Analysis, 2020
Kumar N., Yadav M., Srivastava A.K., Yadav P.N., Saharan V. "Selective Androgen Receptor Modulators: A Novel Approach to Androgen Therapy" – Pharmaceutical Research, 2022
Mazzola V., Defazio G., Botrugno O.A., et al. "Severe Drug-Induced Liver Injury Following the Use of SARMs" – Frontiers in Pharmacology, 2020
Christiansen A.R., Lipshultz L.I., Hotaling J.M., Pastuszak A.W. "Selective androgen receptor modulators: the future of androgen therapy?" – Translational Andrology and Urology, 2020
Solt L.A., Wang Y., Banerjee S., et al. "Regulation of circadian behaviour and metabolism by synthetic REV-ERB agonists" – Nature, 2012
Burris T.P. "Nuclear hormone receptors for heme: REV-ERBalpha and REV-ERBbeta are ligand-regulated components of the mammalian clock" – Molecular Endocrinology, 2008
Kanayama G., DeLuca J., Meehan W.P., et al. "Ruptured Tendons in Anabolic-Androgenic Steroid Users: A Cross-Sectional Cohort Study" – The American Journal of Sports Medicine, 2015
Araujo A.B., Dixon J.M., Suarez E.A., et al. "Clinical review: Endogenous testosterone and mortality in men: a systematic review and meta-analysis" – Journal of Clinical Endocrinology & Metabolism, 2011
U.S. Food and Drug Administration "Warning on Body-Building Products Marketed as Containing Steroids or Steroid-Like Substances" – FDA Safety Alert, 2017 – https://www.fda.gov/
Endocrine Society "Position Statement on Androgen Therapy" – Journal of Clinical Endocrinology & Metabolism, 2019
European Medicines Agency "Public statement on unauthorized medicines containing SARMs" – https://www.ema.europa.eu/
World Anti-Doping Agency "Prohibited List 2024" – https://www.wada-ama.org/
Brainum J. "SARMs Harm" – Applied Metabolics, 2025 – https://www.appliedmetabolics.com/sarms-harm-by-jerry-brainum-5-25/
Brainum J. "SARMs: A Failed Promise?" – Applied Metabolics, 2024 – https://www.appliedmetabolics.com/sarms-a-failed-promise-by-jerry-brainum-9-24/
PubMed Central – National Library of Medicine – https://pubmed.ncbi.nlm.nih.gov/




